
Understanding the distinctions between disc extrusion and sequestration is vital for accurate diagnosis and effective treatment of spinal disorders, particularly when interpreting MRI findings. These differing types of disc herniations can significantly affect patient care strategies and outcomes. With over 35 years of clinical experience, experts like Dr. Sylvain Desforges emphasize the importance of precise evaluation and patient-tailored therapy in managing such complex spinal conditions. His dedication to evidence-based practice and his leadership roles in Canadian osteopathy and alternative medicine underscore the necessity of combining advanced imaging techniques with holistic clinical expertise.
Spinal disc pathology is a common source of back pain and neurological symptoms, often requiring detailed imaging assessments to guide management choices. MRI remains the gold standard for visualizing intervertebral disc abnormalities, offering unparalleled insight into tissue composition, location, and possible nerve involvement. However, interpreting MRI results can sometimes be challenging due to overlapping features between different types of herniations and other spinal lesions, like tumors.
This article delves into the specific characteristics of disc extrusion and sequestration as seen on MRI, highlighting the clinical significance of distinguishing these entities. Case studies illuminate the potential for misdiagnosis and underscore the critical role of multidisciplinary expertise in spinal care. Through intricate description and practical illustrations, readers will better appreciate how spinal MRI findings correlate with anatomical changes in herniated discs and why nuanced understanding translates into superior patient outcomes.
Detailed MRI Characteristics of Disc Extrusion Versus Sequestration
Disc extrusion and sequestration represent progressive stages of intervertebral disc herniation that differ primarily in the continuity of the herniated disc material with the parent disc and its movement within the spinal canal. Recognizing these differences aids clinicians in prognosis and treatment planning.
- Disc Extrusion: In extrusion, the inner nucleus pulposus breaks through the annulus fibrosus but remains connected to the main disc. MRI typically shows a disc fragment protruding beyond the disc space with a narrow base.
- Disc Sequestration: Sequestration occurs when a fragment of herniated disc completely separates from the parent disc and migrates within the epidural space. This free fragment is often displaced cranially, caudally, or laterally.
The physiological composition of discs—rich in water, particularly in the nucleus pulposus—reflects in MRI signal intensities: the nucleus shows high T2-weighted signal due to hydration and is isointense or hypointense on T1-weighted images. As degeneration progresses, these signals alter, aiding in identifying the disc’s pathological state.
Specific MRI features for extrusion include:
- Irregular disc contour with material extending beyond the disc space.
- Continuity with parent disc can be visualized, although sometimes tenuous.
- T2-weighted image hyperintensity at the herniated disc portion due to fluid content.
Sequestration visualization requires noting:
- A detached free fragment located, typically, within the anterior epidural space but possibly migrating posteriorly.
- No continuity with the originating disc visible superiorly or inferiorly.
- Variable MRI intensity depending on hydration and inflammatory responses.
- Peripheral rim enhancement on contrast-enhanced MRI due to reactive inflammation and neovascularization.
Advanced MRI modalities, including 3D SPACE and contrast-enhanced sequences, enable more precise differentiation by highlighting the fragment’s anatomy and relationship to surrounding tissues. This is crucial given that free fragments may mimic neoplastic lesions, leading to potentially erroneous interventions.
| Feature | Disc Extrusion | Disc Sequestration |
|---|---|---|
| Connection to parent disc | Maintained | Absent (fragment detached) |
| Location | Extends beyond disc space but localized | May migrate freely within epidural space |
| MRI T2 signal | Hyperintense area correlating with hydrated disc material | Variable, often hyperintense but dependent on hydration and inflammation |
| Contrast-enhancement pattern | Usually none or minimal | Peripheral rim enhancement due to inflammatory reaction |
Such careful analysis steers therapy toward conservative options like spinal decompression when appropriate or surgical intervention when nerve compression symptoms intensify.

Clinical Implications and Diagnostic Challenges of Disc Sequestration Mimicking Spinal Tumors
Disc sequestration presents a diagnostic conundrum because free disc fragments displaced into the epidural space may resemble spinal tumors on MRI. This generates difficulty in clinical decision-making and necessitates interdisciplinary expertise for accurate diagnosis.
Case studies show patients presenting with symptoms such as:
- Low back pain radiating to lower limbs
- Neurological deficits including numbness and muscle weakness
- Gait disturbances and movement limitations
These symptoms mirror those of spinal tumors, as sequestrated disc fragments can compress the spinal cord or nerve roots. Radiologically, the overlap is notable, with variable signal intensities and contrast enhancement patterns mimicking neoplastic tissue characteristics.
Differential diagnosis involves:
- Reviewing clinical history and symptom evolution: tumor symptoms tend to progress differently than disc-related pain.
- Utilizing advanced MRI sequences: 3D imaging and contrast-enhanced MRI help clarify fragment location and vascular features.
- Correlation with laboratory and neurological evaluations: ruling out systemic or infectious causes that tumors might indicate.
Comprehensive patient evaluation by an expert with deep understanding of spinal biomechanics and pathology, such as Dr. Sylvain Desforges, is indispensable. His methodology includes a detailed clinical examination in conjunction with high-resolution imaging, adhering to strict ethical standards and Quebec’s Collège des médecins medical regulations. This detailed assessment helps avoid unnecessary invasive procedures and paves the way for tailored conservative or surgical care.
| Diagnostic Aspect | Spinal Tumor | Sequestrated Disc |
|---|---|---|
| Symptom duration | Progressive worsening | Often acute or subacute exacerbation |
| MRI enhancement | Often homogeneous or heterogeneous enhancement | Peripheral rim enhancement due to inflammation |
| Fragment Mobility | Fixed mass | May migrate within epidural space |
| Histopathology | Neoplastic cells | Intervertebral disc tissue |
Such discernment ensures that patients receive appropriate management, supported by innovative spinal decompression therapies and minimally invasive interventions at specialized centers like Clinique TAGMED, established by Dr. Desforges and his team.
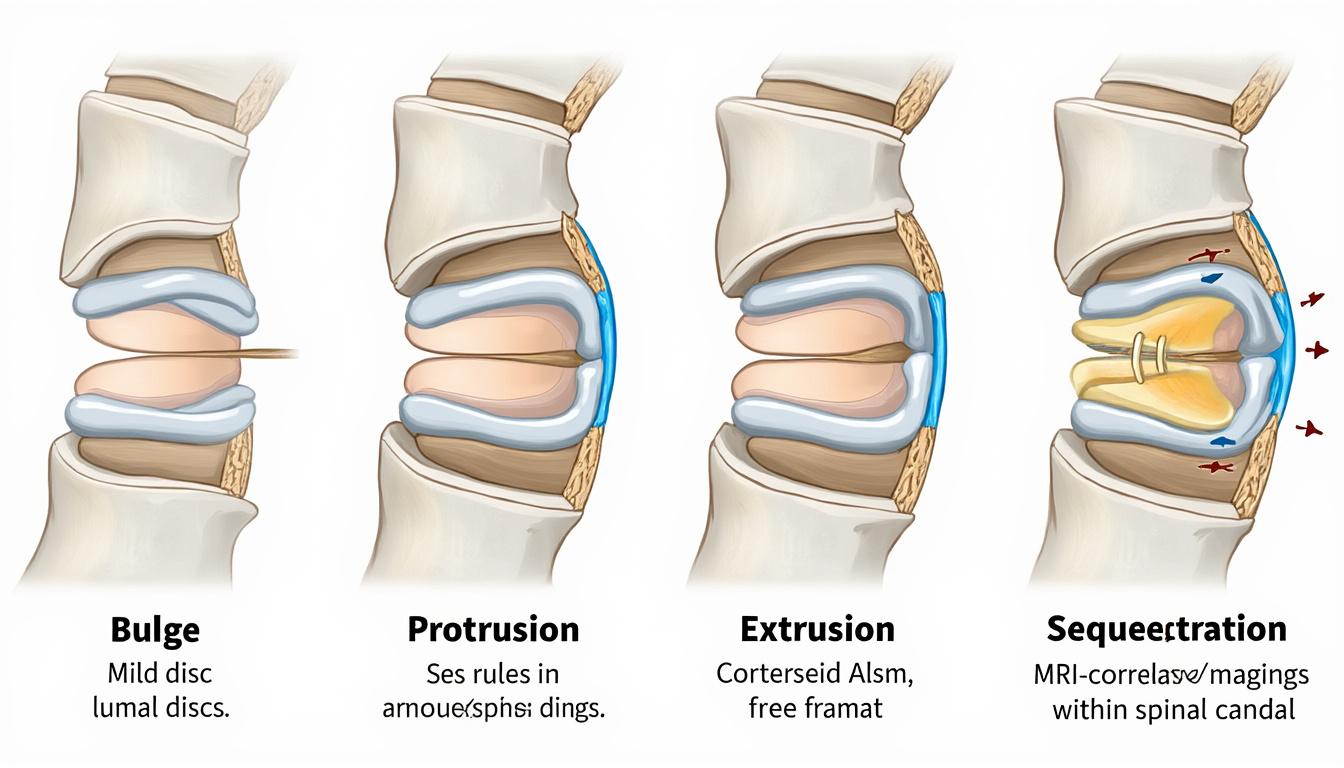
Comparing Disc Herniation Progression: Bulge, Protrusion, Extrusion, and Sequestration
The natural history of disc pathology involves a continuum from minor to severe anatomical disruption, outlined by terms often encountered in MRI reports, which can confuse patients. Understanding these helps clarify prognosis and treatment.
- Disc Bulge: A subtle, symmetric extension of the disc beyond its boundaries without annular rupture, often asymptomatic and age-related.
- Disc Protrusion: The nucleus pulposus pushes the annulus fibrosus outward but remains intact, potentially irritating nerve roots.
- Disc Extrusion: Rupture of the annulus fibrosus with the nucleus escaping but still connected to the disc.
- Disc Sequestration: Free disc fragment separated from the parent disc, representing the most severe form.
Recognition of these stages is essential for risk stratification and therapeutic decisions. Many patients with protrusions or early extrusions achieve relief through non-surgical methods including:
- Non-surgical spinal decompression therapy, alleviating pressure on affected nerves.
- Targeted chiropractic and osteopathic adjustments enhancing spinal mobility.
- Specialized rehabilitation focusing on lumbar stabilization and muscular support.
| Stage | Anatomical Change | Connection to Disc | Potential Symptoms | Treatment Options |
|---|---|---|---|---|
| Bulge | Uniform disc extension | Intact | Often none or mild | Conservative care |
| Protrusion | Focal annular bulging | Intact | Possible nerve irritation | Physical therapy, chiropractic care |
| Extrusion | Ruptured annulus with escaping nucleus | Connected | Moderate to severe pain | Decompression, possible surgery |
| Sequestration | Detached free fragment | Disconnected | Severe pain, neurological deficits | Surgical intervention if conservative fails |
Informing patients with clarity about their specific MRI findings is crucial for empowerment and adherence to treatment plans. Dr. Desforges champions patient education that demystifies technical terminology and fosters collaborative decision-making.
Advanced Imaging Technologies Enabling Precise Spine Pathology Differentiation
Modern spine care increasingly leverages cutting-edge imaging technologies, driven by innovation from global industry leaders like Siemens Healthineers, GE Healthcare, Philips Healthcare, Canon Medical Systems, and Hitachi Medical Systems. These advancements underpin superior diagnosis accuracy and personalized treatment plans.
- 3D SPACE MRI sequences: Provide 3-dimensional isotropic imaging for finer visualization of disc fragments and their spatial relationships.
- Contrast-Enhanced MRI: Helps differentiate disc fragments from tumors by detecting peripheral rim enhancement patterns indicative of inflammatory neovascularization.
- High-Resolution T2-Weighted Imaging: Enables better detection of hydrated nucleus pulposus material versus dense fibrous tissues.
- Dynamic Spinal Imaging: Offers functional insights into segmental motion and instability.
- Emerging Laser Therapy Integration: Enhances non-invasive treatment options when combined with precise imaging guidance.
Furthermore, companies like Medtronic, Zimmer Biomet, Stryker, Boston Scientific, and Fujifilm Healthcare contribute to sophisticated spinal implants and non-surgical decompression devices, forming the backbone of modern spine care facilities like Clinique TAGMED.
Through collaboration with such technological innovators, clinicians gain the ability to tailor interventions precisely, minimizing patient risk while maximizing therapeutic benefit. This integration also aligns with rigorous scientific standards and medical regulations, as followed by Dr. Sylvain Desforges.
| Technology | Purpose | Key Advantages | Industry Leaders |
|---|---|---|---|
| 3D SPACE MRI | Detailed 3D imaging of spinal structures | High resolution, allows slice reformation in any plane | Siemens Healthineers, GE Healthcare |
| Contrast-Enhanced MRI | Differentiating inflammatory lesions from tumors | Highlights peripheral vascularity | Philips Healthcare, Canon Medical Systems |
| Dynamic Imaging | Assessment of spinal motion and stability | Functional data beyond static imaging | Hitachi Medical Systems |
| Laser Therapy Guidance | Non-invasive treatment accuracy | Precision targeting with minimal collateral damage | Medtronic, Boston Scientific |
| Spinal Implants | Structural support and motion preservation | Customized, minimally invasive | Zimmer Biomet, Stryker, Fujifilm Healthcare |
Personalized Patient Care in Managing Disc Extrusion and Sequestration
For patients diagnosed with disc extrusion or sequestration, a personalized care approach is paramount, recognizing the uniqueness of each case and the complexity of spinal mechanics. The clinical expertise of professionals, exemplified by Dr. Sylvain Desforges, ensures that every patient receives thorough evaluation and an individualized treatment roadmap.
- Comprehensive clinical assessment: Detailed history, neurological exam, and functional evaluations guide subsequent imaging requisitions.
- Collaborative interpretation: Multidisciplinary review of MRI findings with radiologists and spine surgeons refines diagnosis.
- Tailored conservative interventions: Including spinal decompression therapy with devices similar to DRX9000, combined with osteopathic manipulations and targeted rehabilitation.
- Regular monitoring and outcome tracking: Using patient-reported outcomes and serial imaging.
- Clear communication and education: Patients are empowered with understandable explanations about their condition and treatment options.
This approach harmonizes scientific rigor with a compassionate, motivational tone, reinforcing that patients deserve care based on best available evidence and technologies. It also avoids premature surgical interventions unless clinically justified, thereby reducing risks and promoting recovery.
| Step in Personalized Care | Description | Benefit to Patient |
|---|---|---|
| Initial Evaluation | Comprehensive history and physical exam under expert guidance | Identifies precise clinical issues and symptom drivers |
| Imaging Interpretation | Expert analysis of MRI with focus on extrusion vs sequestration | Raises diagnostic accuracy and guides therapy |
| Conservative Therapy | Non-invasive treatments like spinal decompression and osteopathy | Promotes healing and symptom relief without surgery |
| Surgical Referral | Careful consideration for surgery when neurological compromise exists | Ensures timely and appropriate intervention |
| Follow-up and Education | Patient engagement with education and progress tracking | Improves adherence and long-term spine health |

Key Differences in Symptomatology and Management Strategies
Disc extrusion and sequestration often lead to overlapping symptoms but have subtle differences influencing clinical decisions. Pain, typically manifesting as low back discomfort radiating along a nerve root, may evolve as follows:
- Disc Extrusion Symptoms: Pain localized near the affected disc level, sometimes associated with mild to moderate neurological signs, including numbness or tingling due to nerve root irritation but generally preserving motor strength.
- Disc Sequestration Symptoms: Severe pain often coupled with significant neurological deficits including muscle weakness, abnormal sensation, and sometimes impaired reflexes, stemming from the free fragment irritating multiple nerve roots or causing inflammation.
Management considerations balance symptom severity, neurological status, and the likelihood of spontaneous resolution:
- Disc Extrusion: Candidates for conservative care with spinal decompression, physical therapy, and osteopathic interventions. Surgery is reserved for refractory cases or progressive neurological deficits.
- Disc Sequestration: More likely to require surgical removal given risks of persistent compression and inflammation; surgery is often followed by internal fixation and rehabilitation for optimal recovery.
| Aspect | Disc Extrusion | Disc Sequestration |
|---|---|---|
| Pain Severity | Moderate | Severe |
| Neurological Deficits | Mild to moderate | Often significant |
| Treatment | Primarily conservative | Surgical intervention more common |
| Prognosis | Good with conservative care | Favorable post-surgery with rehabilitation |
This nuanced understanding empowers clinicians to design treatment plans that optimize outcomes while minimizing unnecessary risks, synchronized with Dr. Desforges’ patient-centered philosophy emphasizing personalized evaluation.
The Role of Pathological Examination Post-Surgery in Confirming Diagnosis
Despite advances in MRI imaging and expert clinical interpretation, definitive diagnosis between sequestrated disc fragments and spinal tumors often necessitates surgical exploration and pathological examination.
Pathological evaluation confirms the composition of the excised lesion, usually revealing fibrocartilaginous intervertebral disc tissue in cases of sequestration, thus excluding neoplasia or infection. This gold-standard confirmation ensures appropriate post-operative management and patient reassurance.
- Surgical safety and planning: Comprehensive preoperative imaging guides minimally invasive approaches, reducing risks.
- Pathology identifies tissue type: Distinguishing soft disc material from tumor cells influences prognosis and need for adjunct therapies.
- Patient counseling: Accurate diagnosis relieves anxieties about malignancy.
- Postoperative rehabilitation planning: Tailored based on confirmed diagnosis.
- Research insights: Aggregated pathology data improve future diagnostic protocols.
| Benefits of Pathological Confirmation | Details |
|---|---|
| Diagnostic Certainty | Distinguishes disc tissue from malignant or infectious lesions |
| Guide for Treatment | Ensures appropriate therapy post-surgery |
| Patient Reassurance | Clarifies benign nature, reducing unnecessary anxiety |
| Improved Prognosis | Enables tailored rehabilitation strategies |
| Contributes to Clinical Knowledge | Supports refinement of MRI interpretation criteria |
Dr. Sylvain Desforges’ practice at Clinique TAGMED integrates surgical expertise with evidence-based evaluation, emphasizing preoperative diagnostics yet recognizing pathological confirmation as an indispensable part of patient care.
Integrating Non-Surgical and Surgical Treatments in Advanced Spine Care
Effective management of disc extrusion and sequestration often involves a stepped approach, beginning with the least invasive options and advancing to surgical interventions when necessary. Dr. Desforges’ clinical philosophy and extensive experience advocate for exhausting conservative therapies before surgery whenever feasible.
- Non-surgical interventions: Spinal decompression therapy (using devices such as DRX9000), gentle osteopathic adjustments, and targeted physical therapy to reduce disc pressure and alleviate nerve irritation.
- Minimally invasive procedures: Techniques utilizing real-time imaging guidance, reducing tissue trauma and improving recovery time.
- Surgical options: Reserved for persistent symptoms, neurological decline, or imaging evidence of significant nerve root or spinal cord compression, including laminectomy, discectomy, and internal fixation as indicated.
- Post-treatment rehabilitation: Focused on restoring function and preventing recurrence through strength, flexibility, and ergonomic training.
By coordinating multidisciplinary teams and incorporating innovations from medical technology leaders such as Medtronic and Stryker, Clinique TAGMED exemplifies progressive spine care models combining efficacy, safety, and patient comfort.
| Treatment Stage | Approach | When Indicated | Benefits |
|---|---|---|---|
| Conservative | Spinal decompression, osteopathy, physiotherapy | Initial symptoms, mild to moderate nerve irritation | Non-invasive, good symptom relief |
| Minimally Invasive | Image-guided injections, laser therapy | Moderate symptoms, failed conservative care | Lower risk, quicker recovery |
| Surgical | Laminectomy, discectomy, fixation | Severe neurological deficits, refractory pain | Definitive decompression and symptom resolution |
| Rehabilitation | Targeted exercises, education | Post-procedure recovery | Restores function, prevents recurrence |
Empowering Patients Through Clear Education and Personalized Support
Patient understanding of their spinal condition is a cornerstone of effective management. Given the complexity of terms like extrusion and sequestration in MRI reports, simplifying medical jargon is crucial. Dr. Sylvain Desforges prioritizes patient education that unpacks these concepts with clarity and empathy.
- Use of visual aids and analogies: Describing disc extrusion as toothpaste squeezed partially out of a tube and sequestration as a piece of toothpaste broken off, helps patients grasp the nature of their injury.
- Transparent discussion of diagnostic uncertainties: Clarifying why certain findings may mimic tumors and the necessity of comprehensive evaluation.
- Encouragement of questions and dialogue: Building trust and active patient involvement.
- Accessible online resources and follow-up opportunities: Supporting ongoing learning and self-care.
- Personalized care plans: Emphasizing that each patient’s treatment is adapted to their unique presentation and goals.
This educational focus, combined with a reassuring tone and attention to regulatory standards in Québec and Canada, helps mitigate fears and fosters adherence to therapy, ultimately enhancing recovery trajectories.
| Educational Strategy | Purpose | Outcome |
|---|---|---|
| Visual Analogies | Make complex concepts relatable | Improved patient comprehension |
| Clear Communication | Reduce fear about MRI findings | Patient confidence and cooperation |
| Interactive Dialogue | Address patient concerns | Active participation in care |
| Resource Provision | Support self-management | Better long-term outcomes |
| Customized Treatment Plans | Individualize therapy | Enhanced effectiveness and satisfaction |
What is the main difference between disc extrusion and sequestration?
Disc extrusion involves herniated disc material that remains connected to the parent disc, while sequestration means the disc fragment has completely separated and migrated within the spinal canal.
How can MRI help differentiate between a sequestrated disc and a spinal tumor?
MRI, especially with contrast enhancement, shows peripheral rim enhancement in sequestrated discs due to inflammatory reaction, whereas tumors often demonstrate homogeneous or heterogeneous enhancement patterns.
Is surgery always required for disc sequestration?
Not always; however, sequestrated discs causing severe neurological symptoms or failing conservative care typically require surgical removal followed by rehabilitation.
Can conservative treatments relieve symptoms of disc extrusion?
Yes, many patients respond well to non-invasive therapies like spinal decompression, osteopathic adjustments, and targeted physical rehabilitation.
Why is pathological examination important after surgical removal of a spinal lesion?
Pathology confirms the diagnosis by distinguishing disc tissue from tumors or other pathological entities, guiding postoperative treatment and providing patient reassurance.