

Expert Clinical Series | Dr. Sylvain Desforges, osteopath
The Herniated Disc Authority Guide
A Deep Dive into Biomechanical Failure, Recovery Logic, and Why Traditional Rehab Often Fails
Preface: After more than two decades dedicated to non-surgical spinal care, I have seen thousands of patients who arrived at my clinic in more pain than when they started their recovery. The reason? They were treating a structural pressure problem with muscular exercise recipes. This guide exists to correct that clinical error and provide you with a scientific roadmap to real healing.
— Dr. Sylvain Desforges, B.Sc., D.O., N.D.
The Central Thesis
An active herniated disc is not a fitness problem; it is a biomechanical injury involving tissue vulnerability, annular failure, and neurochemical irritation. To recover, the clinical priority is not “getting strong,” but reducing intradiscal pressure to allow the body’s natural healing cascade to take place.
1. The Disc as a Pressurized Vessel
To understand why exercise is dangerous, you must first understand what a disc actually is. It is not a shock absorber made of rubber. It is a hydrostatic pressurized vessel.
The Nucleus Pulposus is composed of a gel-like substance rich in proteoglycans that attract water. This creates internal pressure that pushes outward. The Annulus Fibrosus is made of collagen lamellae that contain this pressure.
In a healthy state, this system is perfect. In a herniated state, the “walls of the vessel” are torn. When you add pressure to a vessel with a broken wall, the contents are forced out through the tear. This is basic physics, yet it is often ignored in traditional physical therapy.
Data Analysis: Relative Intradiscal Pressure
These figures represent the load placed on your lower lumbar discs compared to a neutral standing position.
Lying
Standing
Walking
Sitting
Bending
Crunches
Mechanical Risk
Flexion Spikes: Forward bending increases internal pressure. If you have an annular tear, this load may push the nucleus toward the nerve root.
The Exercise Trap
Crunches & Bracing: A standard abdominal crunch can create high pressure. During an acute herniation, this may behave like squeezing a tube of toothpaste with the cap off.
Stagnation
Prolonged Sitting: Sitting for hours may prevent “imbibition”—the movement of nutrients into the disc—effectively starving the tissue of the resources it needs to repair.
2. The “Toothpaste Effect” and Annular Failure
When an annular tear occurs, it is rarely a single event. It is usually the result of thousands of cycles of micro-trauma. Once the tear is active, the disc loses its ability to distribute weight evenly.
The displaced disc material is not just a mechanical lump. It is a neurochemical irritant. The nucleus pulposus contains inflammatory proteins that, when they touch a nerve root, may create burning, electricity, tingling, or pain down the leg.
Why traditional exercise fails here: Muscular strengthening does not retract this material or stop the chemical fire. By increasing the squeeze on the disc, exercises may keep inflammatory proteins leaking toward the nerve.
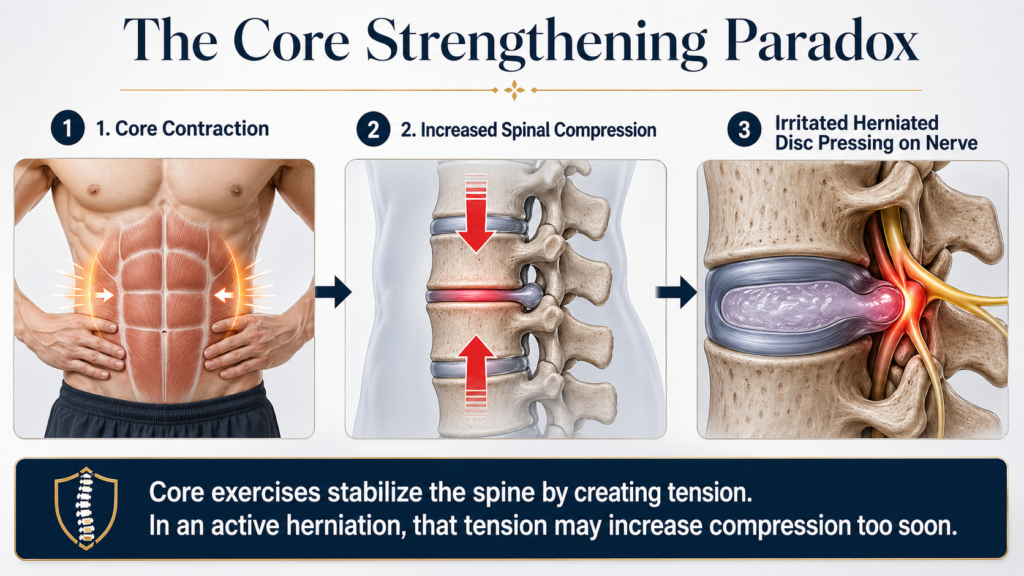
3. Deconstructing the “Core Strength” Myth
Every patient is told: “You need a stronger core.” While true for prevention, it is often mistimed advice in the acute phase of a herniated disc.
The Axial Loading Conflict: Core exercises like planks or bird-dogs require co-contraction. This means the muscles around your spine squeeze at once to create stability. That squeeze creates axial compression. If your disc cannot tolerate its own internal pressure, adding muscular compression may aggravate the lesion.
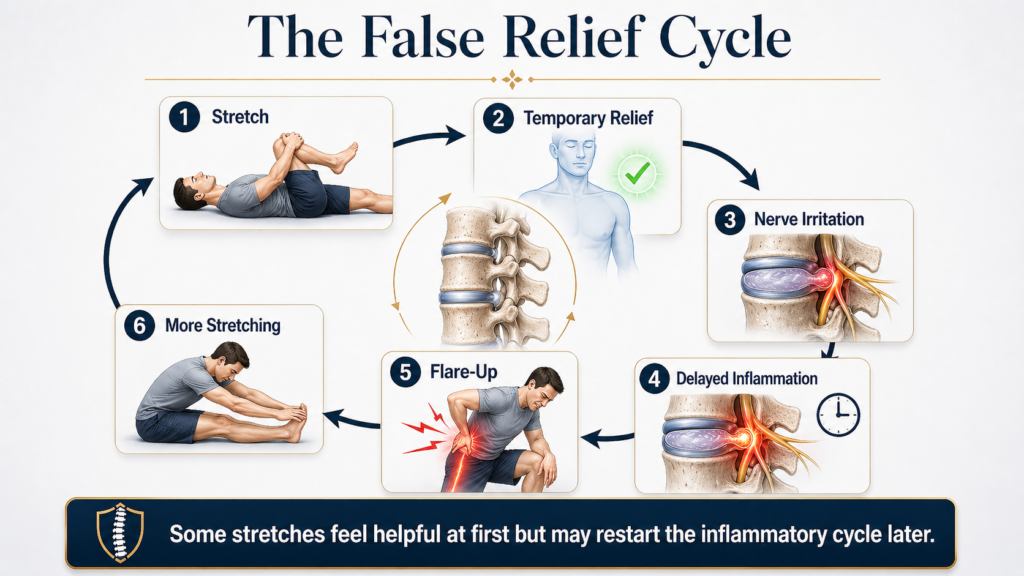
The Stretching Deception
Patients often stretch their hamstrings because their leg feels tight. This tightness may be a protective neurological reflex. When you stretch it, you may tug on an inflamed nerve. You might feel temporary sensory relief, but later the pain may return with a vengeance. This is the delayed flare-up cycle.
High-Risk Movements to Stop Immediately
Lumbar Flexion (Bending Forward)
The Biomechanics: Flexion opens the back of the vertebrae and compresses the front, forcing the disc gel backward toward the nerve.
Common Culprits: Putting on socks, reaching into the dishwasher, pelvic tilts, and sit-ups.
Rotation Under Load (Twisting)
The Biomechanics: Rotation may shear annular layers, especially when combined with load.
Common Culprits: Shoveling snow, Russian twists, or reaching for a heavy bag in the back seat of a car.
Sustained Axial Compression
The Biomechanics: Continuous gravity without movement can create a state of creep where the disc loses height and becomes more vulnerable.
Common Culprits: Long-distance driving, standing still for hours, or sleeping on an unsupportive mattress.
4. The Philosophy: Space First, Movement Later
The biological timeline for disc healing cannot be rushed, but it can be supported. Our clinical approach focuses on three pillars:
- Unloading (Decompression): Creating negative pressure inside the disc to encourage the herniated material to move away from the nerve.
- Imbibition: Restoring the pump mechanism that brings oxygen and nutrients into the avascular disc tissue.
- Centralization: Guiding movement so that leg pain moves back toward the spine, indicating the nerve is no longer under the same threat.
The Authority Recovery Sequence
Each phase has a different clinical focus.
Phase 1: Protection
Mechanical Calm & Decompression
- Decompression treatments to lower internal pressure
- Short frequent walks
- Ice to manage neurochemical inflammation
- Strict avoidance of prolonged sitting
Phase 2: Stabilization
Isometric Neutral Stability
- Safe nerve gliding techniques
- Isometric core engagement without spinal movement
- Postural correction for daily activities
Phase 3: Loading
Progressive Resilience
- Functional weight-bearing exercises
- Progressive resistance training
- Return to sport and hobbies
Clinical Red Flags: When to Stop Reading and Go to the ER
A herniated disc can occasionally become a medical emergency. If you experience any of the following, seek immediate medical evaluation:
- Sudden loss of bowel or bladder control.
- Saddle anesthesia: numbness in the groin or inner thighs.
- Progressive foot drop: inability to lift your toes or foot.
- Sudden, severe weakness in both legs.
Final Word: Your Roadmap to Resilience
Healing a herniated disc is not about doing more; it is about doing the right things at the right time. If you are currently stretching, bracing, and exercising but your pain remains or travels down your leg, you may be working against your own biomechanics.
Stop the cycles of micro-trauma. Create the space your disc needs. Then, and only then, rebuild the strength to protect your future.
Ready to move from “Managing Pain” to “Biomechanical Recovery”?
Why Traditional Exercises Can Be Dangerous for a Herniated Disc
A Biomechanical Guide by Dr. Sylvain Desforges, Herniated Disc Treatment Expert for More Than 20 Years
Most patients with back pain receive the same advice: strengthen your core, stretch your hamstrings, stay active, and begin therapeutic exercises as soon as possible. For a simple muscular strain, that advice may be reasonable. Muscles often respond well to progressive movement because they have a rich blood supply and a strong capacity to repair when loaded correctly.
A herniated disc is different. It is not simply a weak back, a tight muscle, or a posture problem. It is a mechanical injury involving one of the most pressure-sensitive structures in the spine. When the outer wall of the disc is weakened or torn, the wrong movement at the wrong time can increase pressure inside the disc, irritate the nerve root, and prolong the inflammatory cycle.
The question is not whether movement is good or bad. The real question is whether the injured disc is ready to tolerate that movement.
At SOS Herniated Disc, our approach is based on a simple principle:
Before a damaged disc can be strengthened, it must first be protected, decompressed, and stabilized.

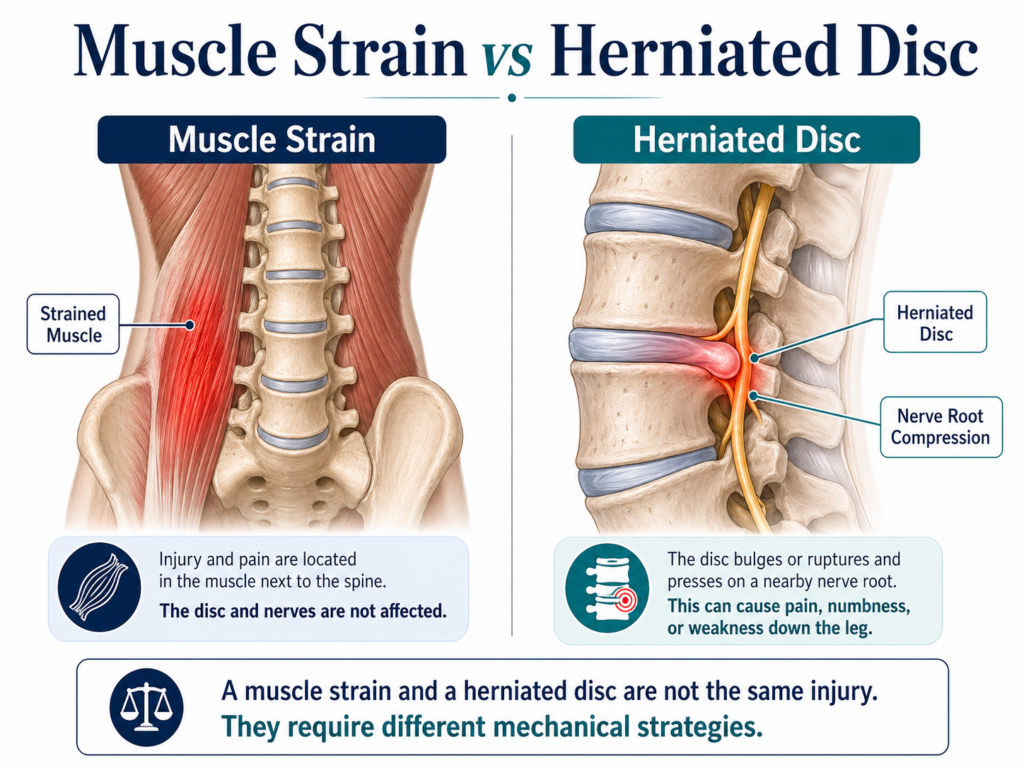
1. A Herniated Disc Is Not a Simple Back Strain
One of the most common mistakes patients make is treating a herniated disc as if it were a simple muscle strain. This misunderstanding often leads them to stretch harder, exercise more, or “push through” discomfort in an attempt to recover faster. Unfortunately, this can have the opposite effect.
A muscular strain usually involves irritation or small tears in muscle fibers. These tissues are highly vascularized, meaning they receive a good blood supply. Because of this, they often respond well to gentle movement, circulation, progressive loading, and gradual strengthening.
A herniated disc behaves differently. The spinal disc has a limited blood supply and depends heavily on pressure changes and fluid exchange for nutrition. It is designed to absorb load, but when its outer ring is damaged, it becomes vulnerable to the very forces it normally manages well.
The spinal disc is made of two major parts. The outer ring, called the annulus fibrosus, is made of strong layered fibers. It acts like a containment wall. The inner portion, called the nucleus pulposus, is softer and more gel-like. It behaves like a hydraulic cushion, distributing pressure through the spine during movement and loading.
When the annulus weakens or tears, the nucleus can migrate outward. If the disc material bulges or herniates toward a nerve root, the patient may experience back pain, leg pain, sciatica, numbness, tingling, burning sensations, or weakness.
Key Clinical Difference
| Simple Back Strain | Herniated Disc |
|---|---|
| Usually involves muscles or ligaments | Involves the intervertebral disc |
| Often improves with movement | May worsen with the wrong movement |
| Good blood supply | Limited direct blood supply |
| Usually local pain | May cause sciatica, numbness, tingling, weakness |
| Often tolerates stretching | Stretching may irritate the nerve root |
| Strengthening may help early | Strengthening may compress the injured disc too soon |
Patient-Friendly Explanation
A muscle strain often needs movement to recover. A herniated disc may first need reduced pressure. This distinction is critical. A patient with a disc injury should not automatically be placed into a standard back exercise program without first understanding the disc’s mechanical tolerance.
Bullet Summary
A herniated disc is not simply:
- A weak core problem.
- A tight hamstring problem.
- A general posture problem.
- A simple muscular strain.
- A condition that should automatically be stretched or strengthened.
A herniated disc may involve:
- A tear or weakness in the annulus fibrosus.
- Migration of the nucleus pulposus.
- Increased intradiscal pressure.
- Nerve root irritation.
- Local inflammation.
- Protective muscle spasm.
- Sciatic pain or neurological symptoms.
2. The “Pressurized Vessel” Reality
To understand why certain exercises can aggravate a herniated disc, we must understand intradiscal pressure. The disc is not a passive piece of cartilage. It acts like a pressurized hydraulic structure. Every time a person bends, lifts, sits, twists, coughs, strains, or contracts the abdominal wall, pressure inside the disc changes.
In a healthy disc, these pressure changes are normal. The disc absorbs force and distributes it across the spinal segment. However, when the annulus is torn or weakened, pressure becomes more dangerous. The nucleus pulposus tends to move toward the path of least resistance. If there is already a fissure, bulge, or herniation, increased pressure can push the disc material further toward the compromised area.
A simple analogy is a balloon with a weak spot. If the balloon is intact, pressure spreads evenly. But if one area is damaged, squeezing the balloon does not repair the weak spot. It forces pressure toward it. In the spine, this same concept helps explain why certain exercises can worsen symptoms when introduced too early.
Many traditional exercises increase intradiscal pressure. Crunches, sit-ups, squats, deadlifts, leg press, loaded bending, twisting exercises, and some yoga postures can all increase mechanical stress on the disc. These movements may be acceptable in a healthy spine or in a later rehabilitation phase. But in an active herniation, they can be poorly tolerated.
This is where many traditional programs fail. They focus on movement before restoring the conditions that make movement safe. The patient is asked to strengthen before the disc has calmed down. The patient is asked to stretch before the nerve has become less irritable. The patient is asked to stabilize before the injured tissue can tolerate compression.
TAGMED’s existing clinical content emphasizes that compression, bending, lifting, twisting, prolonged sitting, and certain exercises may increase stress on an injured disc and potentially aggravate symptoms.
Disc Pressure Analogy Table
| Analogy | Disc Reality |
|---|---|
| Balloon with a weak spot | Disc with a weakened annulus |
| Squeezing the balloon | Increasing spinal compression |
| Pressure moves toward the weakness | Nucleus migrates toward annular tear |
| More squeezing worsens the bulge | More loading may worsen disc symptoms |
| Stop squeezing first | Reduce pressure first |
Movements That Commonly Increase Disc Stress
| Movement or Activity | Why It Can Be Risky |
|---|---|
| Crunches | Lumbar flexion + abdominal compression |
| Sit-ups | High flexion demand and disc pressure |
| Squats | Axial compression and bracing |
| Deadlifts | Compression + hip hinge load |
| Leg press | High lumbar compression, especially if pelvis rounds |
| Toe-touch stretching | Lumbar flexion and neural tension |
| Twisting yoga poses | Rotation through damaged annular fibers |
| Prolonged sitting | Sustained disc loading |
| Heavy lifting | Compression and shear forces |
| Jogging | Repetitive impact through the spine |
Bullet Summary
In an active herniated disc, the priority is to reduce:
- Intradiscal pressure.
- Nerve root irritation.
- Mechanical friction.
- Excessive spinal compression.
- Repeated flexion and rotation.
- Protective muscle spasm.
The treatment sequence should be:
- Reduce pressure.
- Calm the nerve.
- Restore safe motion.
- Rebuild strength later.

3. Why “Core Strengthening” Can Backfire During an Active Herniation
“Strengthen your core” is one of the most common recommendations given to people with back pain. The advice is not always wrong. Long-term spinal health often requires good trunk endurance, pelvic control, and coordinated muscle activation. A stable core can help protect the spine when the body is ready for that type of work.
The problem is timing. During an active herniated disc episode, the spine may not be ready for core strengthening. The disc may be chemically inflamed, mechanically compressed, and neurologically reactive. In that state, asking the patient to brace, contract, plank, crunch, or stabilize can increase compression across the injured spinal segment.
Core exercises work by creating muscular tension around the spine. This tension can be useful later because it improves control. But in the early phase, that same tension can increase load. The abdominal wall, spinal extensors, diaphragm, pelvic floor, and deep stabilizers can all contribute to internal pressure and spinal compression when activated strongly.
This creates a biomechanical conflict. A disc that needs decompression is being compressed. A nerve that needs less irritation is being exposed to more movement, tension, or pressure. Muscles that are already guarding may be asked to contract even harder.
This is why some patients feel worse after exercises that appear simple or safe. They may say, “The exercise did not hurt while I was doing it, but later my sciatica became worse.” Others report that their back tightens, locks, or spasms after a core routine. These reactions are often signs that the disc and nerve were not ready for that level of mechanical demand.
Core Exercises: Risk by Phase
| Exercise | Acute Herniation Phase | Later Stabilization Phase |
|---|---|---|
| Crunches | Usually high risk | Often still unnecessary |
| Sit-ups | High risk | Usually avoided or modified |
| Plank | May be too compressive | May be useful if tolerated |
| Bird-dog | May irritate if unstable | Often useful later |
| Dead bug | May be modified carefully | Useful if neutral spine maintained |
| Squat | Often too compressive | Reintroduced progressively |
| Deadlift | Usually inappropriate early | Advanced progression only |
| Leg press | Often high compression | Reintroduced cautiously, if at all |
Warning Signs That Core Exercises Are Too Early
Core strengthening may be inappropriate if the patient experiences:
- Pain traveling farther down the leg.
- Increased sciatica after exercise.
- Back locking or spasming later in the day.
- Increased symptoms in sitting.
- Burning, numbness, or tingling after exercise.
- Pain that returns stronger several hours later.
- Morning-after flare-ups.
- A need to take more medication after exercising.
Key Principle
Core strengthening is not wrong. Premature core strengthening is wrong.
A herniated disc must earn the right to be loaded again.
4. Stretching: Why Temporary Relief Can Be Misleading
Many patients with a herniated disc feel tightness in the lower back, hamstrings, glutes, or hips. Naturally, they assume they should stretch. This seems logical because stretching often produces a sensation of relief. The patient feels a pull, the muscle seems to loosen, and for a short time the body may feel better.
However, in disc-related pain, what feels like muscle tightness is not always a muscle problem. The sensation may come from nerve irritation, dural tension, protective muscle guarding, or inflammation around the nerve root. In these cases, stretching may not be addressing the real cause of the symptoms.
A patient with sciatica, for example, may feel tightness down the back of the leg. This is often interpreted as a hamstring problem. But the sciatic nerve travels along a similar pathway. If the nerve is irritated, a hamstring stretch may also tension the nerve. What feels like a muscle stretch may actually be a neural tension stress.
This is why some patients feel better during the stretch but worse afterward. During the stretch, the nervous system may experience temporary distraction. The muscle may relax briefly. The patient may feel that something has been released. But if the stretch irritated the nerve root or increased tension through the dural system, the inflammatory response may develop later.
A typical pattern is very common. The patient stretches and feels temporary relief. One or two hours later, the tightness returns. Later that day, the sciatica becomes sharper. By evening or the next morning, the patient is in a flare-up and cannot understand why.
Stretching Reaction Timeline
| Time After Stretching | Possible Patient Experience | What It May Mean |
|---|---|---|
| During stretch | Feels good, pulling sensation, temporary relief | Neurological distraction or temporary muscle relaxation |
| 30–90 minutes later | Tightness returns | Underlying irritation remains |
| 2–4 hours later | Sciatica or back pain increases | Inflammatory response may be building |
| Later that evening | Burning, tingling, or spasm | Nerve may be irritated |
| Next morning | Flare-up, stiffness, worse leg pain | Stretch may have exceeded tissue tolerance |
Stretches That Commonly Cause Problems
| Stretch | Potential Problem |
|---|---|
| Toe-touch stretch | Lumbar flexion + neural tension |
| Hamstring stretch | May tension the sciatic nerve |
| Knee-to-chest | Lumbar flexion may stress posterior disc |
| Seated forward fold | Flexion under sustained load |
| Deep yoga twist | Rotation through injured annulus |
| Piriformis stretch | May irritate sciatic pathway if too aggressive |
| Child’s pose | Deep lumbar flexion may not be tolerated |
| Downward dog | Hamstring and neural tension combined |
Bullet Summary
Stretching may be risky when:
- The pain travels below the knee.
- The patient has numbness or tingling.
- Symptoms worsen after sitting.
- The stretch produces leg symptoms.
- Relief is temporary but flare-ups occur later.
- The patient feels worse the next morning.
- The stretch involves flexion, rotation, or nerve tension.
Key Principle
Relief during a stretch does not prove that the stretch is helping the disc.
The true test is how the patient feels several hours later and the next day.
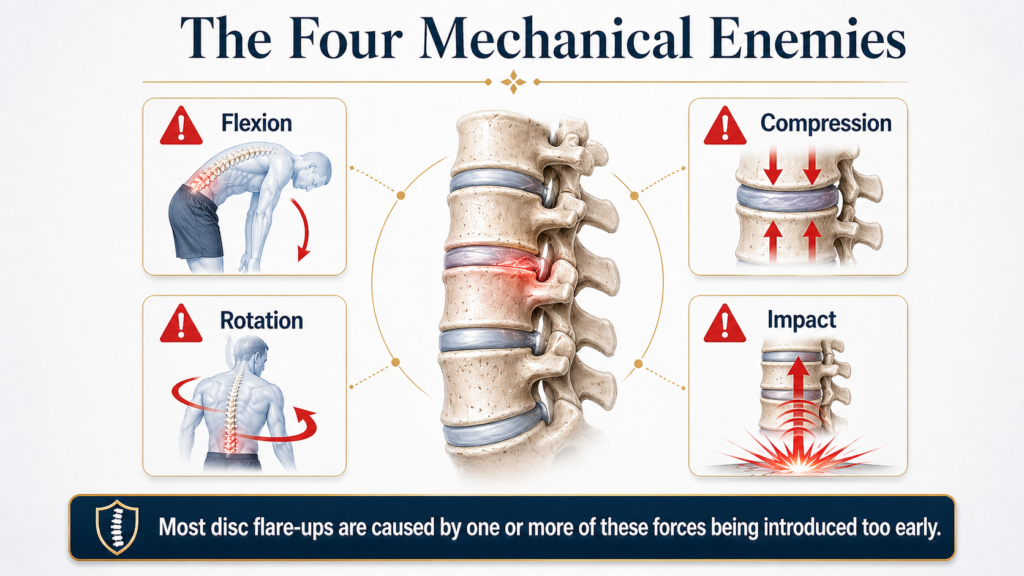
5. The Four Mechanical Enemies of an Active Herniated Disc
During the active phase of a herniated disc, not all movements carry the same risk. Four mechanical forces are especially important: flexion, compression, rotation, and impact. These forces are not always harmful in a healthy body. They are part of normal life and normal athletic function. But when the disc is injured, inflamed, or unstable, they must be carefully controlled.
Flexion means bending forward. This includes touching the toes, rounding the back, sitting slumped, tying shoes in a curled posture, picking objects up from the floor, or performing knee-to-chest movements. Flexion changes how pressure is distributed inside the disc. In many lumbar herniations, especially posterior or posterolateral herniations, repeated or loaded flexion may increase stress on the already weakened posterior annulus.
Compression is the second mechanical enemy. Compression occurs when spinal segments are pressed together. It happens during lifting, carrying, prolonged sitting, bracing, heavy exercise, and even sustained postures. Compression is normal in daily life, but excessive compression on an injured disc may increase symptoms.
Rotation is the third major concern. Rotation means twisting. The annulus fibrosus is made of layered fibers arranged in different directions. This design helps the disc resist torsion. But when the annulus is already damaged, twisting can create shear stress across the injured fibers.
Impact is the fourth enemy. Impact includes jogging, jumping, running on hard surfaces, skipping rope, contact sports, and sudden landings. Each impact sends force upward through the legs, pelvis, and spine. In a healthy spine, this may be tolerated. In an inflamed disc with nerve irritation, repetitive impact can increase symptoms.
The TAGMED herniated disc content similarly warns against heavy lifting, bending, twisting, jogging, jump rope, contact sports, golf, cycling in flexion, yoga, and other activities that may increase stress during recovery.
The Four Mechanical Enemies
| Mechanical Force | What It Means | Common Examples | Why It Matters |
|---|---|---|---|
| Flexion | Bending forward | Toe touches, slumped sitting, laundry, knee-to-chest | May increase posterior disc stress |
| Compression | Loading the spine | Lifting, squats, leg press, planks, heavy carrying | May increase intradiscal pressure |
| Rotation | Twisting the spine | Golf, yoga twists, vacuuming, turning while lifting | May stress annular fibers |
| Impact | Repetitive force through spine | Jogging, jumping, contact sports, rope skipping | May irritate inflamed disc and nerve |
Risky Daily Activities
| Daily Activity | Hidden Mechanical Risk | Safer Early Strategy |
|---|---|---|
| Picking laundry from floor | Flexion + load | Ask for assistance or use raised baskets |
| Vacuuming | Repeated rotation | Move feet instead of twisting trunk |
| Feeding pets | Forward bending | Raise bowls temporarily |
| Long driving | Prolonged sitting compression | Short breaks every 30–45 minutes |
| Carrying groceries | Compression + uneven load | Lighter loads, both hands balanced |
| Gardening | Flexion + rotation | Avoid during acute phase |
| Golf | High-speed rotation | Wait until stable |
| Jogging | Impact | Begin with short flat walks if tolerated |
| Yoga | Flexion and twisting | Avoid deep poses early |
| Cycling | Sustained lumbar flexion | Avoid if symptoms worsen |
6. Why Exercise Can Worsen Sciatica
Sciatica is not simply back pain that travels into the leg. It usually indicates irritation of the sciatic nerve or one of the nerve roots that contributes to it. When a herniated disc irritates or compresses a nerve root, the nervous system becomes more sensitive. Movements that would normally be harmless can suddenly become painful.
An inflamed nerve behaves differently from a healthy nerve. It may react to compression, stretch, vibration, chemical inflammation, or friction. This explains why patients with sciatica can be aggravated by movements that appear gentle. A mild hamstring stretch may tension the nerve. A simple walk may become too much if the distance is excessive. A basic core exercise may increase pressure around the irritated segment.
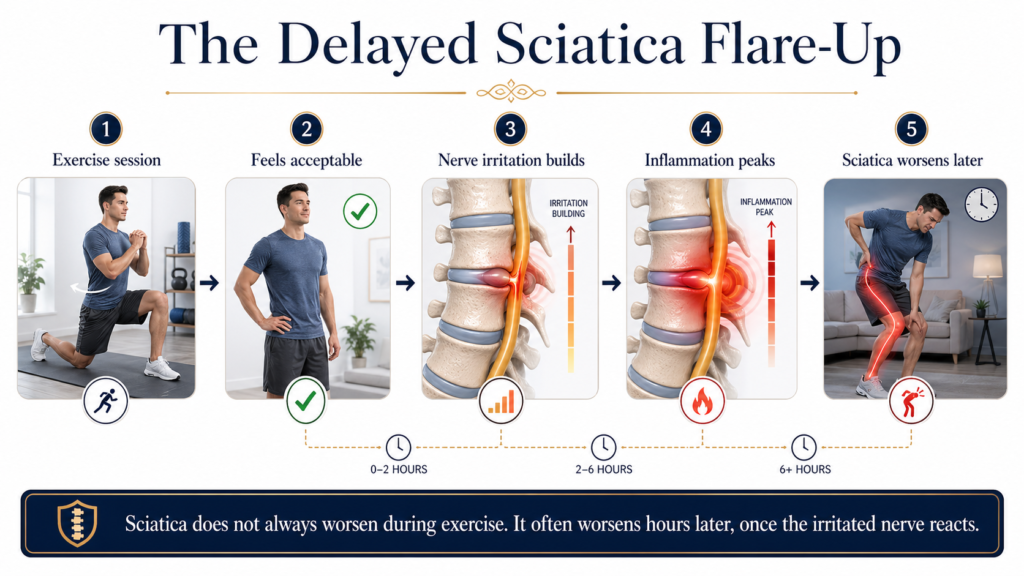
The difficulty is that nerve irritation does not always react immediately. A patient may complete an exercise session and feel acceptable. Then, several hours later, the leg pain becomes sharper. The patient may feel more burning, tingling, or numbness. The back may tighten. The next morning, symptoms may be worse.
This delayed flare-up is one of the most important clinical clues in disc-related sciatica. It means that the exercise did not necessarily fail because it was done incorrectly. It may have failed because the nerve was not ready for that mechanical demand.
Sciatica can also worsen when exercise causes the disc material to rub, press, or move near the nerve root. Even small repeated movements may irritate a hypersensitive nerve. Once the inflammatory response increases, the patient may enter a cycle of pain, spasm, guarding, and reduced mobility.
Signs That Exercise May Be Worsening Sciatica
Exercise may be too aggressive if it causes:
- Pain traveling farther down the leg.
- Increased numbness or tingling.
- Burning pain after movement.
- Symptoms that worsen in sitting.
- Pain with coughing or sneezing.
- Back locking or spasming after exercise.
- Symptoms that appear two to four hours later.
- Worse pain the next morning.
- New or progressive weakness.
Sciatica Irritation Table
| Symptom Pattern | Possible Interpretation |
|---|---|
| Pain moves from back into buttock | Nerve irritation may be increasing |
| Pain travels below the knee | Radicular involvement may be present |
| Tingling increases after stretching | Neural tension may be excessive |
| Sitting worsens symptoms | Disc pressure may be provocative |
| Exercise feels fine, then pain increases later | Delayed inflammatory response |
| Back spasms after activity | Protective guarding may be triggered |
| Leg weakness increases | Requires urgent clinical attention |
Exercise Categories in Active Sciatica
| Exercise Type | Early Phase Risk | Comment |
|---|---|---|
| Hamstring stretching | Moderate to high | May tension sciatic nerve |
| Crunches | High | Flexion and compression |
| Planks | Variable | May be too compressive |
| Bird-dog | Variable | Requires control; may irritate if unstable |
| Walking | Low to moderate | Only if symptom-limited |
| Jogging | High | Repetitive impact |
| Yoga | Variable to high | Depends on flexion and twisting |
| Cycling | Moderate to high | Sustained flexion may aggravate symptoms |
| Swimming | Variable | Avoid excessive lumbar arching or twisting |
| Heavy lifting | High | Compression and bracing |
Key Principle
A patient with active sciatica does not need a harder exercise program. The patient needs a more precise mechanical strategy.
The priority should be to:
- Reduce pressure on the injured disc.
- Calm the irritated nerve root.
- Avoid repeated flare-ups.
- Identify safe positions.
- Reintroduce movement gradually.
- Delay strengthening until the disc and nerve are less reactive.
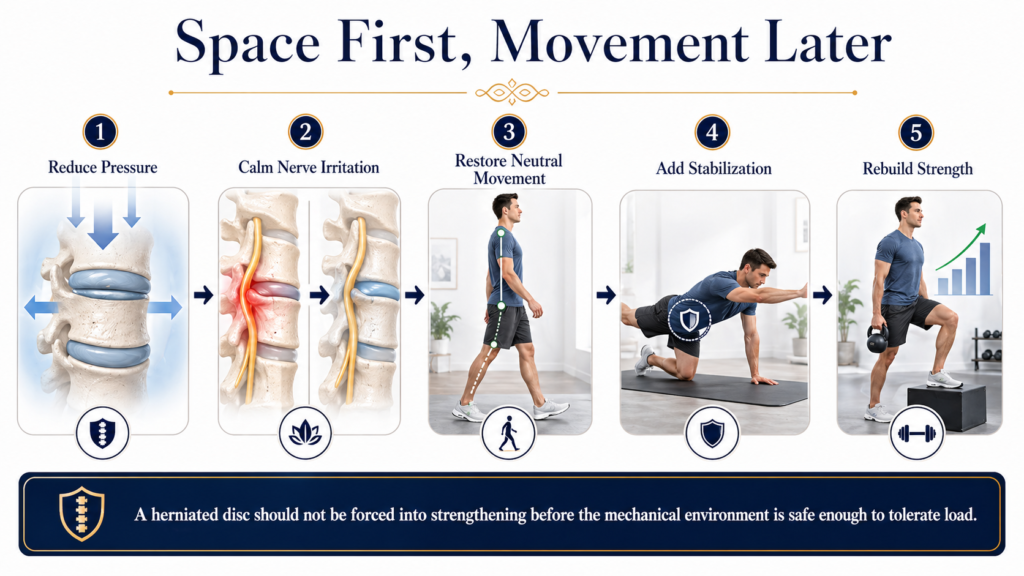
7. Our Philosophy: Space First, Movement Later
At SOS Herniated Disc, we do not avoid exercises because we are against movement. We avoid premature loading because we respect the biomechanics of a damaged disc.
A herniated disc is not simply a movement problem. It is a pressure problem, a tissue tolerance problem, and often a nerve irritation problem. If the treatment plan begins by loading the spine before reducing pressure, the patient may repeatedly flare up and lose confidence in recovery.
This is why our philosophy is simple:
Space first. Movement later.
The first objective is to reduce mechanical stress on the disc. The second objective is to calm the irritated nerve root. The third objective is to restore safe mobility. Strengthening comes later, once the disc and nerve can tolerate progressive loading.
Many patients want to begin exercise immediately because they are afraid of becoming weak. That fear is understandable. However, there is a difference between avoiding harmful loading and becoming inactive. The early phase is not about bed rest or complete immobility. It is about choosing positions and movements that do not repeatedly increase disc pressure or nerve irritation.
In other words, we are not trying to stop the patient from moving. We are trying to stop the patient from moving in ways that keep reopening the problem.
The Treatment Logic
| Traditional Exercise-First Logic | Space-First Biomechanical Logic |
|---|---|
| Strengthen the core immediately | Reduce disc pressure first |
| Stretch tight muscles | Determine whether tightness is muscular or neural |
| Push through mild discomfort | Avoid reproducing nerve symptoms |
| Move more to recover faster | Move only within tissue tolerance |
| Treat all back pain similarly | Match treatment to the disc’s mechanical stage |
| Focus on weakness | Focus first on pressure, inflammation, and nerve irritation |
Why “Space” Matters
The disc sits between two vertebrae. When that space is compressed, the disc is exposed to greater internal pressure. When the disc is already damaged, this pressure can contribute to irritation. The goal of decompressive care is to reduce that mechanical load and create a more favorable environment for healing.
The concept of “space” is not abstract. It refers to reducing compression around the disc and nerve root. When pressure is lowered, the irritated nerve may become less reactive. When the nerve becomes calmer, the muscles may guard less. When the muscles guard less, movement becomes easier. Only then does strengthening become more logical.
What We Prioritize First
In the active phase of a herniated disc, the first priorities are:
- Reduce intradiscal pressure.
- Decrease mechanical irritation around the nerve root.
- Avoid positions that centralize pressure into the injured disc.
- Limit flexion, compression, rotation, and impact.
- Calm protective muscle spasm.
- Improve tolerance to basic daily activities.
- Restore confidence in safe movement.
What Comes Later
Once symptoms are more stable, the priorities shift. The patient gradually begins to rebuild:
- Controlled spinal mobility.
- Postural endurance.
- Neutral spine awareness.
- Gentle stabilization.
- Hip and pelvic control.
- Walking tolerance.
- Progressive strength.
- Return to work, sport, and daily function.
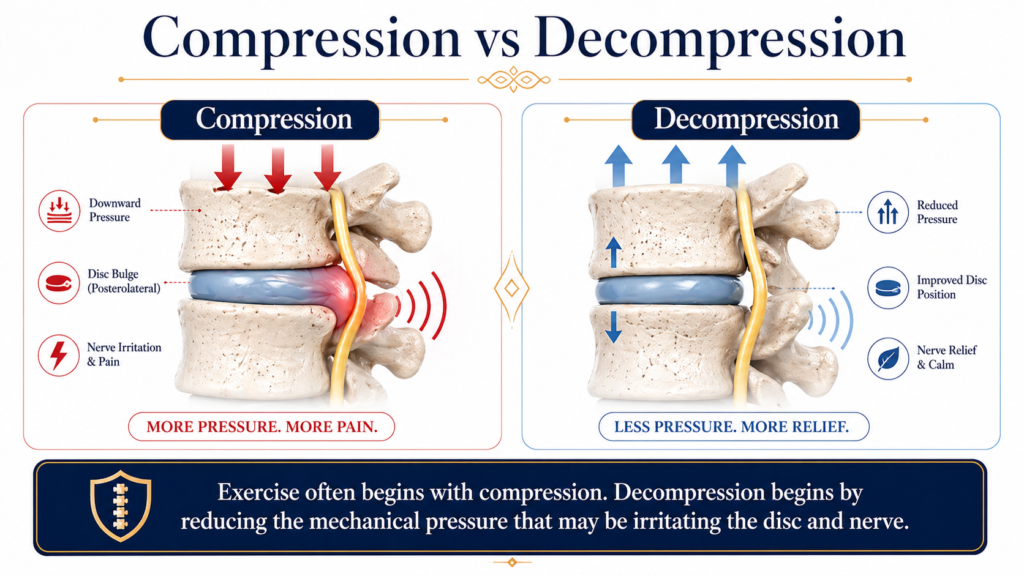
8. Why Decompression Makes More Biomechanical Sense Than Compression
Traditional exercise often begins by asking the body to contract, brace, stabilize, and load. In a healthy spine, that can be useful. In an actively herniated disc, it may be the wrong mechanical message.
A damaged disc usually does not need more compression at the beginning. It needs less. This is the fundamental reason decompression may be more logical than exercise-first rehabilitation for selected patients with active disc symptoms.
During spinal decompression, the goal is to apply a controlled traction force to the spine. This is designed to reduce pressure inside the disc, create a more favorable pressure gradient, and decrease irritation around compressed or inflamed nerve structures. The treatment is not based on forcing movement. It is based on reducing mechanical load.
This is very different from asking a patient to perform abdominal bracing or strengthening exercises while the nerve root is still irritated. Those exercises may have value later, but they can be premature when pain is sharp, radiating, inflammatory, or easily aggravated.
TAGMED’s clinical documents describe neurovertebral decompression as a non-surgical and non-invasive approach using controlled traction to reduce internal disc pressure and relieve compressed nerves. This principle fits directly with the “space first” model.
Compression vs Decompression
| Compression-Based Activity | Decompression-Based Strategy |
|---|---|
| Crunches | Controlled unloading |
| Sit-ups | Reduced intradiscal pressure |
| Heavy lifting | Reduced nerve irritation |
| Squats and deadlifts | Improved mechanical tolerance |
| Prolonged sitting | Better disc fluid exchange |
| Bracing exercises | Less protective guarding |
| High-impact activity | Gradual return to safe movement |
Why Decompression May Help Selected Disc Patients
The purpose of decompression is to change the mechanical environment around the disc. This may assist recovery by reducing the pressure that pushes disc material outward, decreasing irritation on the nerve root, and allowing the body to move away from a constant protective spasm response.
The treatment does not “force” the disc to heal. Rather, it aims to create a more favorable condition in which healing can occur. This distinction matters because no ethical treatment should promise a guaranteed cure. The objective is to improve the environment around the injured tissue so the body has a better chance to recover.
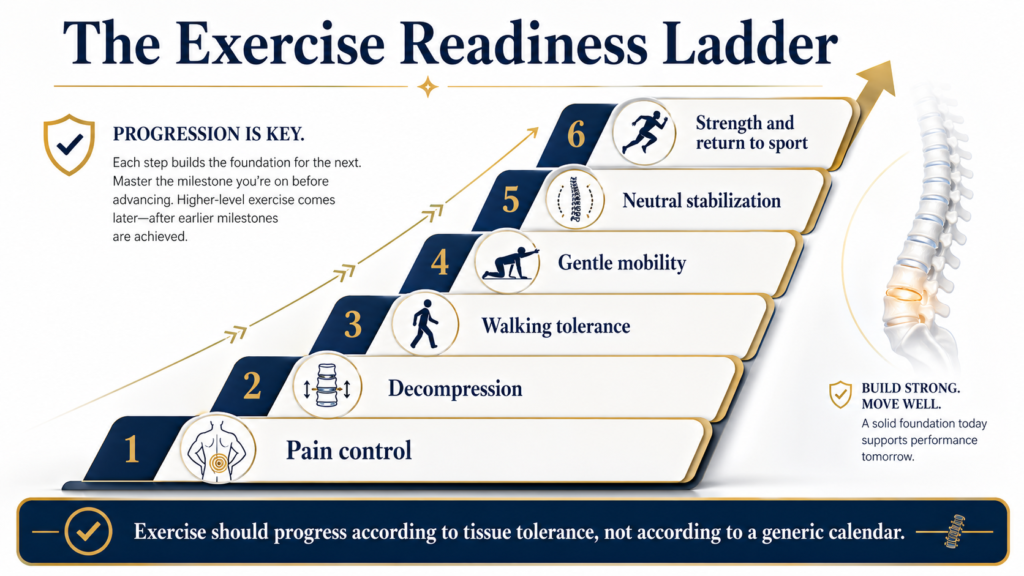
The Biomechanical Sequence
| Step | Goal | Clinical Meaning |
|---|---|---|
| 1. Reduce pressure | Lower mechanical stress | Disc is less compressed |
| 2. Calm nerve irritation | Reduce sensitivity | Sciatica may become less reactive |
| 3. Improve mobility tolerance | Restore basic movement | Patient moves with less guarding |
| 4. Add neutral stabilization | Rebuild control | Spine learns to stabilize without flare-up |
| 5. Progress strength | Restore function | Patient returns to activity safely |
Why This Differs From Generic Exercise Advice
Generic exercise advice often assumes that back pain is caused by weakness, stiffness, or poor conditioning. That may be true for some patients, but it is incomplete for disc herniation. In a herniated disc, the immediate problem may be pressure, inflammation, nerve irritation, and mechanical instability.
A patient cannot always strengthen their way out of a pressure problem. Sometimes the pressure must be addressed first.
9. When Exercise Becomes Safe Again
Exercise is not the enemy. In fact, exercise eventually becomes an important part of recovery for many patients. The problem is not movement itself. The problem is movement introduced before the disc and nerve are ready.
The safest approach is not to ask, “Which exercise is best for a herniated disc?” The better question is, “At what stage is this herniated disc, and what can it tolerate today?”
Exercise becomes more appropriate when the patient’s symptoms are stable, the nerve is less irritable, and daily activities no longer trigger repeated flare-ups. This does not mean the disc is fully healed. It means the patient may be ready for carefully selected movement.
The transition back to exercise should be gradual. A patient should not jump from severe sciatica to planks, squats, or gym workouts. The body must progress through stages of tolerance.
Signs That Exercise May Be Safer to Reintroduce
Exercise may be considered when:
- Leg pain is decreasing.
- Symptoms are no longer traveling farther down the leg.
- Numbness or tingling is improving or stable.
- Sitting tolerance has improved.
- Walking does not trigger delayed flare-ups.
- The patient can sleep with less pain.
- Spasms are less frequent.
- Daily activities are easier.
- Symptoms are not worsening the next morning.
- Clinical evaluation confirms improved mechanical tolerance.
Signs That Exercise Is Still Too Early
Exercise may still be premature when:
- Sciatica is sharp or increasing.
- Pain travels below the knee.
- Numbness or tingling increases after movement.
- The patient has new or worsening weakness.
- Sitting remains highly provocative.
- Stretching causes delayed flare-ups.
- Core exercises increase leg symptoms.
- The back locks or spasms after activity.
- The patient is relying heavily on pain medication to tolerate movement.
Recovery Phase Table
| Phase | Primary Goal | What Is Usually Avoided | What May Be Considered |
|---|---|---|---|
| Phase 1: Acute Protection | Calm symptoms | Flexion, lifting, twisting, impact | Positions of relief, short walks if tolerated |
| Phase 2: Decompression | Reduce pressure | Strengthening, aggressive stretching | Decompression, gentle neutral positioning |
| Phase 3: Controlled Mobility | Restore safe motion | End-range flexion or twisting | Gentle pain-free mobility |
| Phase 4: Neutral Stabilization | Rebuild control | Heavy bracing or fatigue-based exercise | Light stabilization in neutral spine |
| Phase 5: Progressive Strength | Restore function | Sudden return to full load | Gradual strengthening and conditioning |
| Phase 6: Return to Activity | Prevent recurrence | Poor technique, overloading | Work, sport, and lifestyle progression |
The Right Exercise at the Wrong Time Is Still Wrong
A bird-dog may be useful later. A modified plank may be useful later. Hip strengthening may be useful later. Walking may be useful early if it is symptom-limited. But even a good exercise can be harmful if introduced at the wrong stage.
Timing is not a minor detail. Timing is the treatment.
10. Everyday Movements That Can Re-Irritate a Herniated Disc
Many patients think they aggravated their disc at the gym, but the real problem often comes from repeated daily movements. A herniated disc can be irritated by small mechanical stresses repeated throughout the day.
The patient may avoid heavy exercise but still bend repeatedly to pick up laundry, sit for long periods, twist while vacuuming, lift grocery bags, or drive for an hour without a break. Each of these activities may seem harmless. Together, they can keep the disc irritated.
This is why education is essential. A patient recovering from a herniated disc must learn not only which exercises to avoid, but also which daily habits increase disc pressure.
Prolonged Sitting
Sitting is often worse than standing for disc patients because it increases sustained pressure through the lumbar spine, especially when the patient slumps. A patient may tolerate sitting for a few minutes but develop symptoms after 30 to 45 minutes.
Driving can be particularly provocative because it combines sitting, vibration, hip flexion, and limited ability to change position.
Bending Forward
Bending is one of the most common daily triggers. Patients often bend to tie shoes, pick objects from the floor, load the dishwasher, make the bed, garden, or feed pets. Even light objects can provoke symptoms if the lumbar spine rounds into flexion.
Lifting and Carrying
Heavy lifting is an obvious risk, but uneven carrying is also important. Carrying a bag on one side can combine compression with side-bending and rotation. This may irritate the disc or increase protective spasm.
Twisting
Twisting while loaded is especially risky. Vacuuming, shoveling, reaching into the car, turning while holding a child, or rotating while lifting a basket can place shear stress through the lumbar discs.
Sleep Position
Poor sleep posture can keep the spine irritated overnight. Sleeping on the stomach may increase lumbar extension and cervical rotation. Side sleeping without support may allow the pelvis to rotate. Back sleeping without knee support may increase tension in some patients.
Daily Activity Risk Table
| Activity | Hidden Risk | Better Early Strategy |
|---|---|---|
| Long sitting | Sustained disc compression | Stand briefly every 30–45 minutes |
| Driving | Sitting + vibration | Use breaks and lumbar support |
| Tying shoes | Lumbar flexion | Bring foot up or use slip-on shoes temporarily |
| Laundry | Repeated bending and lifting | Use raised baskets or assistance |
| Dishwasher | Flexion and rotation | Face the task directly, avoid twisting |
| Vacuuming | Repeated trunk rotation | Step with feet, keep spine neutral |
| Feeding pets | Forward bending | Raise bowls temporarily |
| Groceries | Compression and uneven load | Carry lighter balanced loads |
| Gardening | Flexion, rotation, sustained posture | Avoid during acute phase |
| Snow shoveling | Flexion + rotation + load | Avoid until stable |
| Making the bed | Reaching and flexion | Move around the bed, avoid long reaches |
Red-Light Activities During the Acute Phase
Patients should be especially cautious with:
- Heavy lifting.
- Repeated bending.
- Twisting while carrying.
- Prolonged sitting.
- Jogging or jumping.
- Deep stretching.
- Core bracing exercises.
- Yoga flexion or rotation poses.
- Golf swings.
- Shoveling.
- Moving furniture.
- Long car rides without breaks.

11. The Exercises We Commonly Recommend Avoiding Early
Not every patient is the same, and no exercise should be judged without context. However, in active disc herniation, certain movements are repeatedly associated with flare-ups. These are not necessarily “bad exercises” for everyone. They are often bad choices for a disc that is still inflamed or mechanically unstable.
The early phase requires restraint. The patient should avoid testing the disc repeatedly. Every flare-up can reinforce pain, increase guarding, and reduce confidence. The objective is to build a calm baseline before adding challenge.
Exercises Often Avoided in the Early Phase
| Exercise | Why It May Be Problematic |
|---|---|
| Sit-ups | Lumbar flexion and high disc pressure |
| Crunches | Flexion with abdominal compression |
| Toe touches | Flexion and neural tension |
| Hamstring stretches | May irritate sciatic nerve |
| Knee-to-chest | Flexes lumbar spine |
| Russian twists | Rotation through injured annulus |
| Deadlifts | Heavy compression and bracing |
| Squats | Axial load and spinal compression |
| Leg press | Lumbar compression, especially if pelvis tilts |
| Jump rope | Repetitive impact |
| Jogging | Repetitive spinal loading |
| Burpees | Flexion, impact, and fatigue |
| Yoga forward folds | Sustained flexion |
| Deep spinal twists | Rotational stress |
| Back extensions | May compress posterior elements in some patients |
Why “Gentle” Does Not Always Mean Safe
Some exercises appear gentle but still create the wrong mechanical force. A slow forward fold is still flexion. A calm yoga twist is still rotation. A light hamstring stretch can still tension the sciatic nerve. A bodyweight squat can still compress the disc.
Safety is not determined only by intensity. It is determined by direction, load, timing, symptom response, and tissue tolerance.

12. What Patients Can Usually Do Instead
A herniated disc recovery plan should not create fear of movement. The goal is to replace provocative movement with safer mechanical choices.
In the early phase, the safest activities are usually those that keep the spine closer to neutral, reduce compression, and do not reproduce leg symptoms. The exact plan must be individualized, but many patients tolerate short, controlled movements better than aggressive stretching or strengthening.
Walking is often useful when it is kept within tolerance. It encourages circulation, reduces fear of movement, and helps the patient avoid prolonged sitting. However, walking should not be forced. If symptoms travel farther down the leg, increase significantly, or flare up later, the duration may be too long.
Neutral positioning is also important. Patients often need to identify positions that reduce symptoms. For some, lying on the back with knees supported may help. For others, side lying with a pillow between the knees may be more comfortable. The goal is to reduce unnecessary stress on the disc while symptoms calm down.
Safer Early Options
| Instead of This | Consider This Early Strategy |
|---|---|
| Jogging | Short flat walking if tolerated |
| Crunches | Neutral rest positions |
| Toe touches | Avoid flexion; use supported movements |
| Hamstring stretching | Gentle nerve-sparing positioning |
| Heavy lifting | Temporary assistance or load reduction |
| Long sitting | Frequent position changes |
| Twisting yoga | Neutral breathing and relaxation |
| Gym workouts | Clinical decompression-first approach |
| Long driving | Breaks, lumbar support, shorter trips |
| Deep squats | Avoid until stable |
Early Movement Rules
A movement is more likely to be acceptable if:
- It does not increase leg pain.
- It does not cause symptoms to travel farther.
- It does not create delayed flare-ups.
- It does not require bracing hard.
- It does not involve deep flexion.
- It does not involve twisting.
- It does not create impact.
- It feels at least as good several hours later.
Key Principle
The right early movement should calm the system, not challenge it.
13. Frequently Asked Questions
“Should I stop all exercise if I have a herniated disc?”
No. The goal is not complete inactivity. The goal is to avoid movements that increase disc pressure or nerve irritation. Many patients can tolerate short walks, neutral positions, and carefully selected movements. However, aggressive strengthening, stretching, lifting, twisting, or impact may need to be avoided during the active phase.
“But I was told to stay active. Is that wrong?”
Staying active is not wrong. The problem is misunderstanding what “active” means. Staying active does not mean doing crunches, deadlifts, yoga twists, long runs, or painful stretches. It may simply mean avoiding bed rest, walking within tolerance, changing positions regularly, and protecting the spine while symptoms calm down.
“Why do I feel better when I stretch?”
Stretching can create temporary relief by reducing muscle tone or distracting the nervous system. But if the stretch increases nerve tension or disc stress, symptoms may return later or worsen. The true test is not how the stretch feels during the movement. The true test is how the body responds later that day and the next morning.
“When can I start strengthening again?”
Strengthening becomes more appropriate when symptoms are stable, sciatica is decreasing, walking and sitting tolerance are improving, and movements no longer trigger delayed flare-ups. The transition should be gradual and based on clinical evaluation, not a fixed timeline.
“Is pain during exercise always bad?”
Pain is information. Mild local discomfort may not always be dangerous, but leg pain, numbness, tingling, burning, worsening sciatica, or delayed flare-ups are warning signs. Pain that travels farther from the spine is especially important and should not be ignored.
“Can a good exercise still be bad for me?”
Yes. A good exercise at the wrong time can be the wrong treatment. Timing, stage of healing, nerve sensitivity, and mechanical tolerance matter more than the name of the exercise.
Suggested FAQ Graphic
Graphic title: Exercise Decision Filter
Visual concept:
A decision tree:
Does it increase leg pain? → Yes → Stop
Does it cause delayed flare-up? → Yes → Modify or avoid
Does it involve flexion, compression, rotation, or impact? → Yes → Evaluate carefully
Does it feel better later and next day? → Possibly acceptable
Caption:
Exercise decisions should be based on symptom behavior, not generic routines.
14. Clinical Safety: When to Seek Urgent Medical Attention
Most herniated disc cases can be managed conservatively, but some symptoms require urgent medical evaluation. Patients should never ignore signs of serious neurological involvement.
Immediate medical attention is required if the patient develops loss of bladder or bowel control, numbness in the saddle area, rapidly worsening weakness, severe progressive neurological symptoms, fever with spinal pain, recent major trauma, unexplained weight loss, or a history of cancer with new severe back pain.
These symptoms may indicate a serious condition that requires medical evaluation beyond conservative care.
Urgent Warning Signs
| Warning Sign | Why It Matters |
|---|---|
| Loss of bladder or bowel control | Possible cauda equina involvement |
| Saddle numbness | Possible serious nerve compression |
| Rapidly worsening leg weakness | Progressive neurological deficit |
| Fever with severe spinal pain | Possible infection |
| Major trauma | Possible fracture |
| Cancer history with new spinal pain | Requires medical evaluation |
| Unexplained weight loss | Possible systemic condition |
| Severe night pain not relieved by rest | Requires further investigation |
15. Final Clinical Message
A herniated disc is not a simple weakness problem. It is a mechanical injury that must be understood before it is loaded. Traditional exercises may help later, but when introduced too early, they can increase pressure, irritate the nerve, and restart the inflammatory cycle.
This is why our approach begins with decompression, protection, and precise evaluation. We do not reject movement. We respect timing.
The goal is not to make the patient move immediately. The goal is to help the disc and nerve calm down so the patient can move again safely.
Our goal is not simply to make you exercise.
Our goal is to help your disc recover enough so movement becomes safe again.